Here is the most useful thing to know before reading another word: if you are carrying more body weight right now, your daily calorie burn is higher — not lower — than a smaller person’s. That is genuinely good news, and it directly affects how you approach fat loss.
Most people assume the opposite. They think a higher body weight means a slower metabolism and that losing weight means eating almost nothing. Neither of those things is true. A heavier body has more tissue to maintain, more mass to move through daily life, and — as a result — a higher Total Daily Energy Expenditure (TDEE). That higher TDEE means your calorie target, even within a fat-loss deficit, can be comfortably higher than you probably expect.
Use the TDEE calculator to get your own accurate starting number — one built around your actual body weight, height, age, and activity level, not a one-size-fits-all estimate designed for someone much smaller than you.
This article covers five things. First, why TDEE is genuinely higher at higher body weights (the physiology behind it, not just the reassurance). Second, how to calculate it accurately. Third, what an appropriate calorie deficit looks like — using a percentage-based approach that works far better than a fixed “subtract 500 calories” rule. Fourth, why recalculating TDEE matters more for this group than any other. And fifth, when involving a doctor adds real value.
Why a Higher Body Weight Means a Higher TDEE
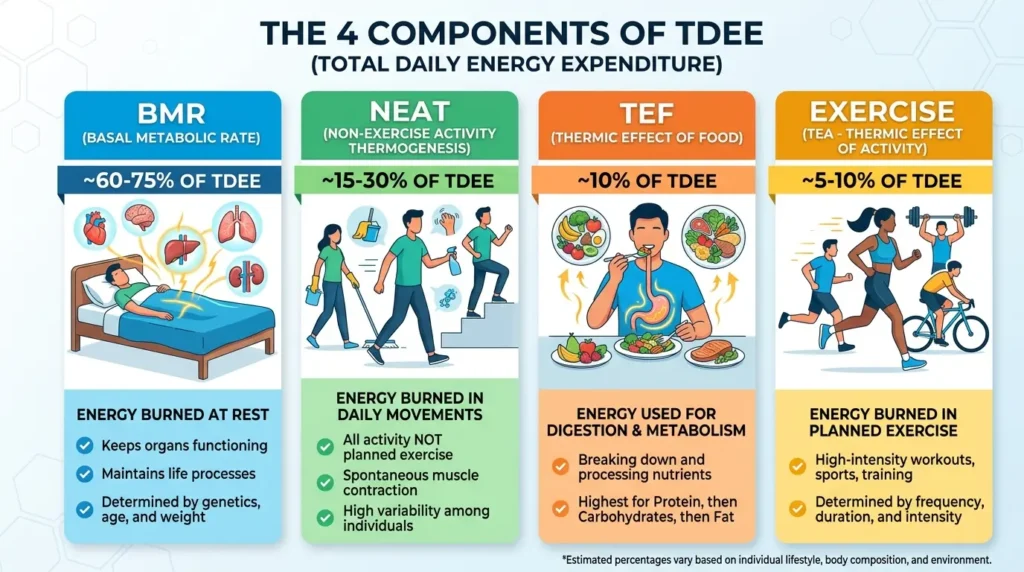
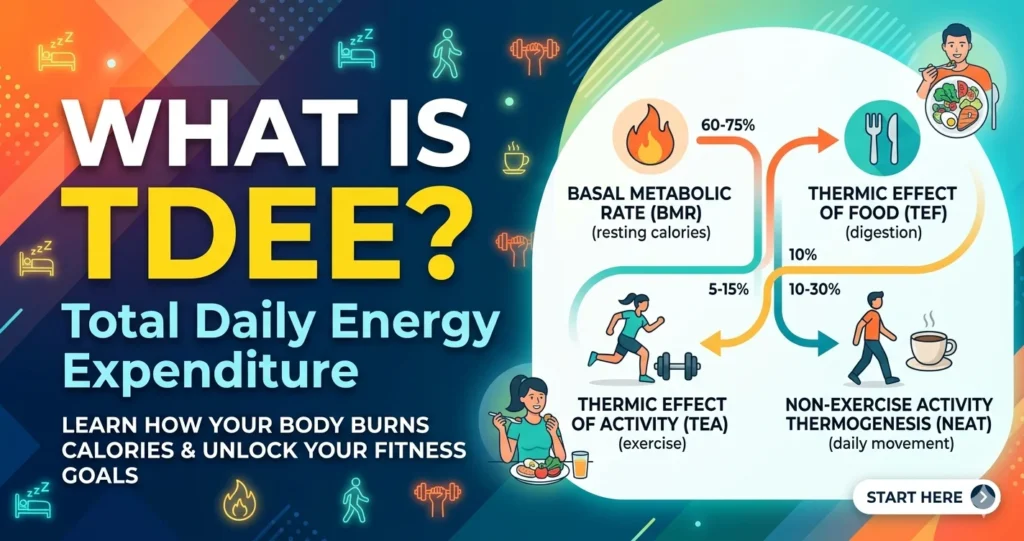
Your TDEE is not just about muscle. The whole body — fat included — costs energy to keep running. Fat tissue (adipose tissue) is biologically active. It has its own blood supply. It produces and responds to hormones like leptin and insulin. It communicates with your brain about hunger and energy availability. Maintaining all of that biological activity requires calories every single day.
On top of that, carrying more body mass changes how hard your cardiovascular system works. Your heart pumps blood to a larger volume of tissue with every beat. Your lungs move air through a larger body. Every organ works a little harder to serve a larger frame — and that extra work shows up as measurably higher resting energy expenditure.
Then there is the movement side of the equation. Walking up a flight of stairs at 110 kg costs more calories than walking the same stairs at 70 kg. This is simple physics — more mass moved against gravity equals more energy used. Even light daily activity burns more calories at a higher body weight, before you add any structured exercise.
Put both together — higher resting metabolic rate and higher activity energy cost — and the result is a meaningfully higher TDEE. This is exactly why the Mifflin-St Jeor equation uses body weight as its main variable. Two people with the same height, age, and sex but different body weights are supposed to get different TDEE values. Both results are correct. The formula is working as designed.
For a deeper look at how BMR and TDEE relate to each other at a biological level, the BMR vs TDEE complete guide covers the full picture.
Worked Comparison — How TDEE Differs at Different Body Weights
Here is what that looks like in real numbers. Same person in every way — 40-year-old woman, 165 cm tall, sedentary lifestyle — except for body weight.
| Body Weight | BMR (kcal) | TDEE — Sedentary (kcal) |
|---|---|---|
| 70 kg | ~1,386 | ~1,663 |
| 90 kg | ~1,586 | ~1,903 |
| 110 kg | ~1,786 | ~2,143 |
Look at the difference between the top and bottom rows. The person at 110 kg has a TDEE roughly 480 calories higher than the person at 70 kg — every single day. That means their fat-loss calorie target, even with a 500-calorie daily deficit, sits at around 1,643 calories. That is more food per day than the 70 kg person eats at full maintenance (1,663 calories).
Read that again. The person at 110 kg, actively losing fat, can eat more daily calories than the lighter person at maintenance. This directly dismantles the “I have to eat almost nothing to lose weight” belief that holds a huge number of people back.
How Many Calories Should an Overweight or Obese Person Eat to Lose Weight?
Skip the fixed numbers. The most accurate, most useful answer here is not “1,200 calories” or “1,500 calories.” Those generic figures were not built around your body weight — they were built around somebody much lighter.
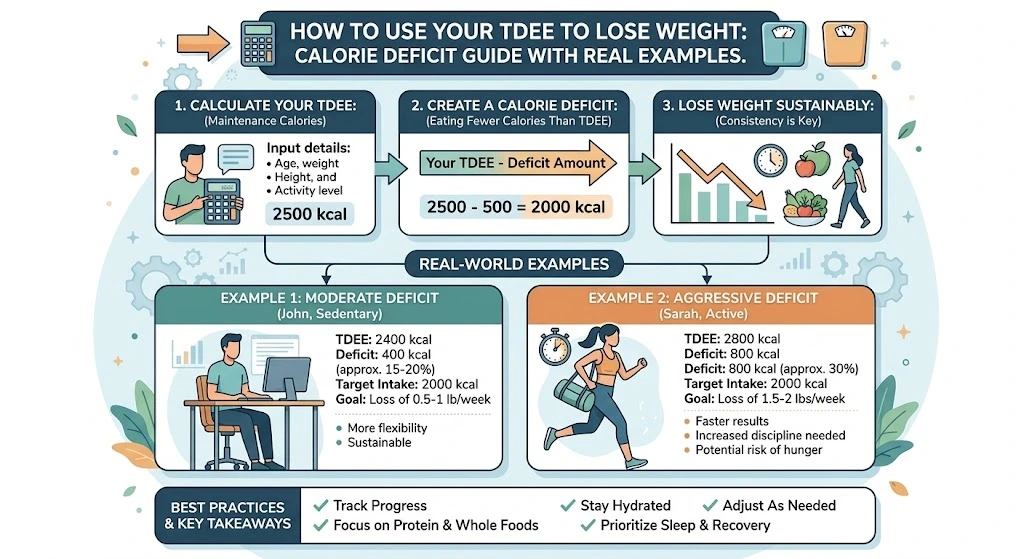
The right framework is percentage-based. Work out your TDEE (using the calculator), then target a deficit that produces 0.5–1% of your current body weight loss per week. This approach scales correctly to any starting body weight, rather than applying the same number to every body size.
NICE — the UK’s National Institute for Health and Care Excellence — recommends a daily deficit of around 600 calories for gradual, sustainable weight loss. That is sensible guidance, but what NICE does not spell out for most people is what 600 calories actually represents as a proportion of their TDEE. For someone burning 1,800 calories a day, a 600-calorie deficit is 33% of TDEE — quite aggressive. For someone burning 2,800 calories a day, that same 600-calorie deficit is only about 21% — moderate and very manageable.
The percentage-based approach automatically accounts for this difference. Here is how it looks in practice for three different starting weights:
| Body Weight | 0.5%/week target | Daily deficit needed | 1%/week target | Daily deficit needed |
|---|---|---|---|---|
| 75 kg | 0.375 kg/wk | ~413 cal/day | 0.75 kg/wk | ~825 cal/day |
| 95 kg | 0.475 kg/wk | ~522 cal/day | 0.95 kg/wk | ~1,045 cal/day |
| 115 kg | 0.575 kg/wk | ~633 cal/day | 1.15 kg/wk | ~1,265 cal/day |
These deficits are calculated using the ~7,700 kcal per kilogram of fat relationship.
Notice how the 95 kg person’s 0.5% target (522 calories/day) is close to the standard “subtract 500” advice — but for the 115 kg person, the same proportional target is 633 calories per day, not 500. And at the 1% upper end, the 115 kg person is targeting a deficit of over 1,200 calories — a figure that sounds large but is fully appropriate and sustainable given their significantly higher TDEE. That is the key insight fixed-number advice misses completely.
Why Larger Deficits Can Be More Sustainable at Higher Starting Weights
This is the part most calorie guides get completely wrong. They apply the same “don’t go above 500 calories deficit” rule to everyone, regardless of starting body composition. That makes sense for a lean person. It is overly cautious — and unnecessarily restrictive — for someone with a meaningfully higher body fat percentage.
Here is why. When you are in a calorie deficit, your body has two places to pull energy from: fat stores and lean tissue (muscle). Which one it prefers depends on availability. When fat stores are abundant — as they are at higher body fat percentages — the body preferentially burns fat rather than cannibalising muscle. The lean mass loss risk associated with aggressive deficits is much more relevant for lean individuals who do not have large fat stores available.
Research on calorie restriction in individuals with obesity (BMI ≥30) has shown that even deficits representing 30% of TDEE produced meaningful improvements in body composition and metabolic markers — including insulin resistance and lipid profiles — over six-week periods, without the lean mass losses that would concern a leaner person on the same proportional restriction.
This does not mean “eat as little as possible.” It means the guidance that applies to a lean person running a 10–15% deficit does not automatically apply here — and that a well-calibrated percentage-based deficit at a higher body weight is both more aggressive in absolute terms and more appropriate than generic guidance suggests.
For the relationship between body composition and calorie targets in more detail, the body recomposition guide explains how fat loss and lean mass preservation interact during a deficit.
How to Calculate TDEE Accurately at Higher Body Weights
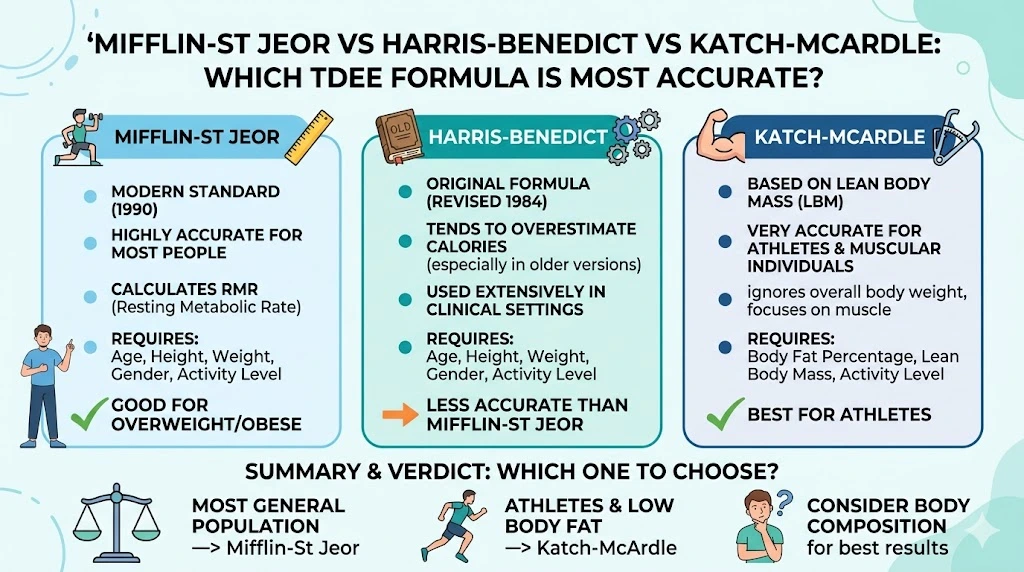
The Mifflin-St Jeor formula is the right choice here. It uses your total body weight directly. It was validated across a broad population that included individuals at higher body weights. And it gives consistently reliable results without requiring any additional body composition measurements.
The Katch-McArdle formula — which is based on lean body mass rather than total weight — sounds more precise, but it is actually less reliable for this audience. Here is the problem: Katch-McArdle needs an accurate body fat percentage measurement to work. At higher body fat percentages, the two most common measurement methods (BIA scales and skinfold calipers) become less accurate. Feeding an unreliable body fat estimate into Katch-McArdle introduces more error than simply using Mifflin-St Jeor with total body weight. Unless you have had a DEXA scan, stick with Mifflin-St Jeor.
For a full breakdown of which formula works best in which situation, the Mifflin-St Jeor vs Harris-Benedict vs Katch-McArdle comparison covers every scenario.
The practical steps:
- Enter your current total body weight (not a goal weight — your actual weight today)
- Enter your height, age, and biological sex
- Select your activity level honestly — most people with desk jobs and no structured exercise should choose sedentary
- Take the TDEE result and apply the percentage-based deficit from the section above
That is the full process. The only meaningful difference from standard TDEE use is the deficit-sizing step — percentage-based rather than a fixed number.
Worked Example — Setting a Calorie Target From TDEE
Let us carry this through with a real person.
Profile: 45-year-old woman, 165 cm tall, 105 kg, desk job, no structured exercise (sedentary).
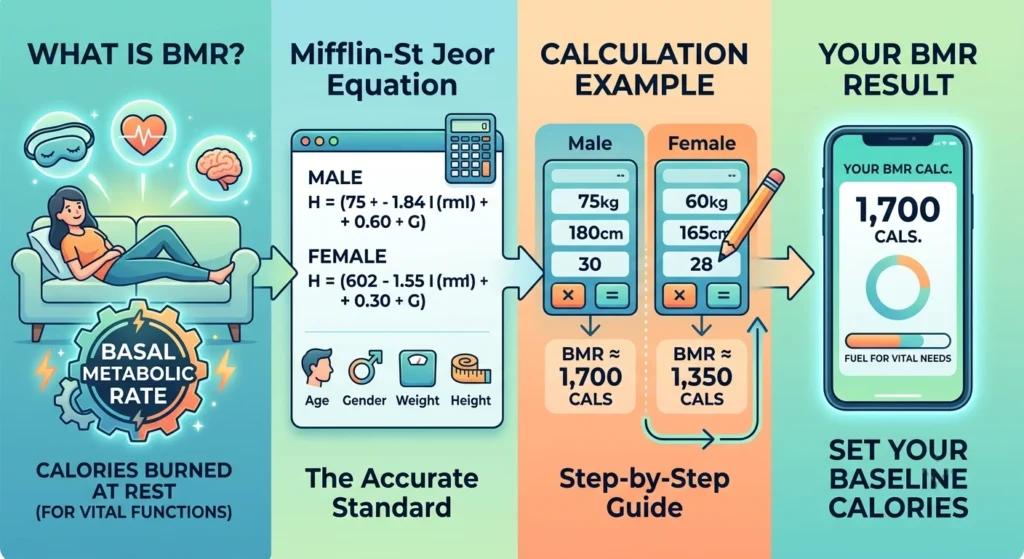
Step 1 — Calculate BMR using Mifflin-St Jeor:
BMR = (10 × 105) + (6.25 × 165) − (5 × 45) − 161
= 1,050 + 1,031.25 − 225 − 161
= 1,695 calories
Step 2 — Apply the sedentary activity multiplier (×1.2):
TDEE = 1,695 × 1.2 = ~2,034 calories per day
Step 3 — Size the deficit using the percentage-based framework:
Target: 0.5–0.75% of body weight loss per week = 0.525–0.79 kg/week
Required daily deficit = ~577–870 calories
Step 4 — Choose a practical target:
A 600-calorie deficit (aligning with NICE guidance and sitting in the middle of the range):
Calorie target = 2,034 − 600 = ~1,434 calories per day
Notice that 1,434 calories is comfortably above the 1,200-calorie floor discussed in guidance around minimum safe calorie intakes. It represents a 29% deficit from TDEE — within the sustainable range for someone at this starting body composition. It is also a real food amount that does not require eating tiny portions or feeling deprived.
For more on how to use TDEE to structure a fat-loss approach from start to finish, the how to use your TDEE to lose weight guide walks through the full method.
Why Recalculating TDEE Matters More for This Group Than Any Other
Here is something almost no calorie guide talks about specifically for this audience: because your TDEE is linked directly to your body weight, and because fat loss at higher starting weights can move faster in absolute terms, your TDEE number changes more quickly and by larger amounts than it does for someone closer to their goal weight.
Set a calorie target in January and ignore it until June, and you may be operating on a number that is 150–200 calories off from where it should be. That might not sound like much — but over time, it is the difference between a meaningful, proportional deficit and a very small one that has quietly stalled your progress.
Let us continue the worked example above. Our 45-year-old woman starts at 105 kg with a TDEE of 2,034 and a daily target of 1,434 calories. She loses 8 kg, bringing her weight to 97 kg. What happens to her TDEE?
New BMR at 97 kg:
= (10 × 97) + (6.25 × 165) − (5 × 45) − 161
= 970 + 1,031.25 − 225 − 161 = 1,615 calories
New TDEE (sedentary, ×1.2):
= 1,615 × 1.2 = ~1,938 calories
Her TDEE has dropped from 2,034 to 1,938 — a fall of nearly 100 calories. If she is still eating 1,434 calories, her deficit has shrunk from 600 calories to just 504 calories. Still meaningful — but the proportional approach (29% of the new TDEE) would now target a deficit of about 562 calories, suggesting a new calorie target of approximately 1,376 calories.
That is a small adjustment — 58 calories — but making it keeps her on a consistent, proportional path rather than unknowingly operating at a shrinking deficit without understanding why progress has started to slow.
Practical rule: Recalculate TDEE every 4–5 kg of weight lost. At higher starting weights, weekly weight loss in absolute kg can be faster than for lighter individuals, so this 4–5 kg threshold may arrive more frequently than you expect. Every time you hit it, go back to the calculator, plug in the new weight, and reapply the same percentage-based deficit to the new TDEE number.
This approach explains why TDEE recalculation frequency matters so much more here than for most other groups. It is not about doing something different — it is about applying the same proportional method to a number that is changing meaningfully as you progress. To understand the weight loss plateau this recalculation helps avoid, the weight loss plateau explained article covers exactly why progress stalls and what to do about it.
When to Involve a Healthcare Professional
Self-directed calorie management at higher body weights is not inherently risky — and nothing in this article requires medical permission to use. That said, professional input adds real value in certain situations, and it is worth knowing what those are.
NICE guidelines suggest a GP consultation is worthwhile for anyone with a BMI above 30 — not because the calorie approach changes, but because a doctor can screen for underlying conditions that affect weight and energy metabolism. Thyroid dysfunction, polycystic ovary syndrome (PCOS), and certain medications can all influence body weight and energy expenditure in ways that make standard TDEE targets less accurate. Identifying these factors before starting means you work with your biology rather than against it.
For individuals of South Asian descent, the relevant BMI threshold is lower — a consultation is recommended from BMI 27.5, reflecting the well-established difference in metabolic risk profile at equivalent body fat percentages between South Asian and other ethnic populations.
Professional oversight becomes particularly important in these specific situations:
- If you are considering a deficit larger than ~35% of TDEE — this threshold is where clinical guidelines flag the need for medical oversight, and where the risk profile changes meaningfully even at higher body fat percentages.
- If your calorie target falls below 800 calories per day — this is the clinical boundary for a very low-calorie diet (VLCD). VLCDs can be medically appropriate and effective, but they require professional supervision.
- If you have existing health conditions — diabetes, cardiovascular disease, kidney issues, or medications affected by significant weight change all warrant care team involvement before major dietary changes.
- If you would benefit from structured support — a GP referral to a weight management programme is a genuinely valuable resource. Many people are unaware these programmes exist or that a referral is available on request.
This section is here to show you where additional support is available and when it adds value — not to suggest you need permission to manage your own nutrition.
Frequently Asked Questions
How many calories should an overweight person eat to lose weight?
There is no single correct number — and any article that gives you one without knowing your body weight, height, age, and activity level is guessing. The right approach is to calculate your personal TDEE using the free TDEE calculator, then apply a deficit targeting 0.5–1% of your current body weight loss per week. For a 95 kg person with a TDEE of around 2,200 calories, this works out to a daily calorie target of roughly 1,200–1,700 calories depending on the rate of loss chosen — but the exact figure depends on individual TDEE, which varies with height, age, sex, and activity level.
How many calories should an obese person eat to lose weight safely?
The same percentage-based framework applies. At higher body weights, this often translates to a larger absolute calorie deficit than standard advice suggests — and this is appropriate and sustainable given the higher starting TDEE. A person with a TDEE of 2,600 calories can target a deficit of 700–900 calories per day (roughly 27–35% of TDEE) while still eating 1,700–1,900 calories daily — well above the commonly cited minimum calorie floors. For BMI above 30 (or 27.5 for South Asian individuals), a GP consultation is recommended by clinical guidelines to screen for underlying factors and provide additional support.
How often should I recalculate my TDEE?
Every 4–5 kg of body weight lost. At higher starting body weights, this point can arrive more quickly than expected because the initial rate of weight loss in absolute kg terms is often faster. Each recalculation involves plugging the new body weight into the TDEE formula and reapplying the same percentage-based deficit — not starting from scratch, just updating the baseline. The complete TDEE beginner’s guide explains how to approach this recalibration step by step.
Why is my TDEE so much higher than my friend’s even though we’re the same height?
Body weight is the dominant variable in TDEE calculation — more so than height in most adult comparisons. Two people of the same height but different body weights will have meaningfully different TDEEs because a heavier body requires more energy both at rest (maintaining more tissue, including metabolically active fat) and in motion (moving more mass through daily activities). This is normal, expected physiology — not a sign of a faster or slower metabolism in the dramatic sense. It also means two people of the same height eating identical calories can have very different outcomes — one might be in a comfortable deficit while the other is at maintenance, purely because of a TDEE difference driven by body weight.
Will my calorie target need to keep decreasing as I lose weight?
Yes — and this is completely normal. As body weight falls, TDEE falls with it. The percentage-based deficit framework handles this automatically: recalculate TDEE every 4–5 kg, reapply the same percentage deficit to the new number, and adjust the calorie target accordingly. This is not “needing to eat less and less forever” — it is recalibrating the same proportional approach to a new, accurate baseline at each stage of the process. The adjustments are usually modest (50–100 calories at a time), and the approach remains consistent throughout. For what happens after you reach your goal weight, the reverse dieting guide explains how to bring calories back up without regaining the weight lost.
Is it harder to lose weight at a higher starting body weight?
In some respects, the opposite is true — at least initially. Higher starting TDEE means a larger absolute calorie deficit is achievable while still eating a comfortable daily food amount. Research suggests that higher body fat percentages allow the body to sustain proportionally larger deficits with less lean mass loss risk compared to leaner individuals on the same proportional deficit. Initial rates of weight loss in absolute kg terms are often faster at higher starting weights. What does require consistent attention is the TDEE recalculation dynamic — because both TDEE and the achievable deficit shrink as weight is lost, the calorie target needs periodic adjustment to maintain the same proportional, sustainable approach throughout.
The Mifflin-St Jeor formula’s accuracy at higher body weights is well supported in the literature — a widely cited validation study published in the Journal of the American Dietetic Association confirmed it performs better across diverse body weights than older formulas like the original Harris-Benedict. Research on TDEE prediction accuracy consistently shows Mifflin-St Jeor as the recommended starting point for clinical and self-directed calorie planning. The NICE CG43 obesity guidelines remain the most cited UK clinical reference for weight management calorie targets and the 600-calorie deficit recommendation discussed throughout this article. For a broad overview of daily calorie needs across different population groups, Healthline’s calorie intake guide provides a well-reviewed general reference.
The macro side of fat loss is just as important as the calorie target. Once you have your TDEE and calorie target set, the calculate macros from TDEE step-by-step guide shows how to split those calories between protein, carbohydrates, and fat in a way that supports fat loss and muscle preservation simultaneously.